35 yo/female patient presents with non-specific LBP. Mild LUQ discomfort is noted. No prior trauma, surgeries, carcinoma or corticosteroid regimen.
AP VIEW LUMBAR APINE. 4 typical lumbar VB are seen. At the lumbosacral junction, a LSTV (lumbar transitional VB) is present with a large spatulated TVP on the right with pseudoarthrosis and associated degenerative change. Did you see the curvilinear density of the LUQ?
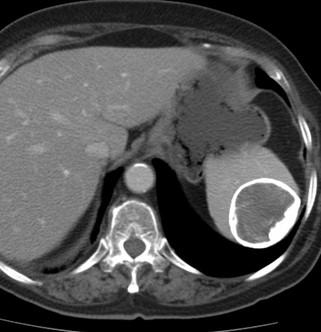
Non-contrast image of the abdomen with calcification within the wall of the splenic cyst.
A cyst larger than 1 cm. in size requires MRI or needle biopsy follow-up. (3)
What do you see?
AP VIEW LUMBAR APINE.
4 typical lumbar VB are seen. At the lumbosacral junction, a LSTV (lumbar transitional VB) is present with a large spatulated TVP on the right with pseudoarthrosis and associated degenerative change.
Did you see the curvilinear density of the LUQ?
XRAY FINDINGS
A ring enhanced radiolucency is present which measured 5.0 cm. on the original DICOM images. This lesion is intra-peritoneal. DX: Splenic cyst.
DISCUSSION: Incidental findings of splenic mass > 1.0 cm. generally are benign (85% of cases). These cystic mass are usually pseudocysts and show no true endothelium on histologic examination but 1/2 of the cases show wall calcification. True epithelial cysts generally show enhancing internal septations & not likely wall calcification. (2) In this case, the 5.0 cm. size, warrants follow-up – either MRI or needle biopsy.